
Character, Personality, and Borderline Dynamics
an interview with Orestis Zavlis

A while ago I wrote an essay about borderline interpersonal/relational processes as part of my attempt to locate what I call “the borderline”. In it, I made mention of Orestis Zavlis. I came across his work in my quest to understand the work of Peter Fonagy, plus we run in the same circles here on Substack.
Orestis Zavlis is a PhD student at the Psychoanalysis Unit in University College London, and his work is focused on critically examining assumptions surrounding the idea of “personality disorder” (see also his Substack, “Personality Disordered,” on the matter).
Mr. Zavlis commented on the essay with some thoughts and a correction. (Probably best to read the essay if you have not; you will get more out of this interview.) I found these very useful, so with his permission I have shared them here. I asked Mr. Zavlis some further questions which he answered, and those are also here. I have done the lightest-touch editing of removing some niceties in our exchanges, plus I have Americanized some of Mr. Zavlis’ spellings for the sake of consistency. Apologies to the Commonwealth. And apologies to Awais Aftab for borrowing his interview format!
I would like to emphasize, particularly for new readers, that I am not a clinician and I don’t have any formal training in any of the psy-disciplines. If my questions and their premises betray a lack of basic knowledge, that’s why. Also, don’t take my words as medical advice, please and thank you!
My thanks to Orestis Zavlis for being so generous with his time, and for raising the academic caliber of this blog!
—Sorbie
Orestis Zavlis: I have many thoughts on the essay but I will restrict myself to three points, all based on specific parts of your essay.
My first point is that your outline of the Zavlis – Fonagy – et al work on “borderline” is very accurate: “Borderline” lives between people. At the same time, though, I would add this: “Borderline” also lives within every person. I think you would agree with this point given your repeated emphasis that we can all enact “borderline” dynamics at times. So, what borderline seems to be, at least in my eyes, is a set of “relational traits” (I don’t like the word “inter-personal”, sorry) that were evolved across the centuries because they were (paradoxically) at least somewhat socially adaptive—maybe because they helped us detect danger (by being suspicious), test loyalty (by being a bit clinging sometimes), and build stronger relationships (by being highly passionate and loving). So, they live to some extent in all of us. And they can be enacted by each of us, particularly in stressful times. The issue is only when they are activated too much and too often, giving the illusion of a “disorder of character or personality” (see my last point).
This leads me to my second point about therapists. Here, I’d say that it’s very unfortunate that some therapists would use theoretical language (particularly from psycho-analysis) to dismiss patients’ perceptions that sometimes (maybe not always and maybe not even mostly, but definitely sometimes) the person who initiates the “cliff-falling” is the therapist themselves because they could not handle a patient’s comment; or because they had a counter-transference reaction; or because they had a bad day; or; or; or… I have written about this previously and criticized prominent figures who engage in this line of reasoning by showing how this line of reasoning is entirely antithetical to true psycho-analysis (because it uses “interpretations” as a defense mechanism), it is deeply unscientific (because it relies on unfalsifiable statements like “you caused me to behave like this through your projective identification”), and, finally and perhaps most importantly, it lacks humility and basic ethics: because at the very least, a therapist should entertain the possibility that since they also have an unconscious life, they may as well, unbeknownst to them, thrown their patient-objects off a cliff and made things worse sometimes (see here).
Finally, and most interestingly, I’d like to briefly comment on your last footnote. According to this footnote “The real live personality disorder is rare, but it is out there.” This is the only statement I’d push back on for the following reason: I think what you may mean here is that these people have a “character disorder” (not a “personality disorder”). I would hate to sound pedantic at this point but I think this distinction matters because DSM-III came and destroyed everything by conflating the idea of “character” with the idea of “personality” but these are not the same thing: Character is about who you are morally speaking (i.e., how you treat others intentionally, ego-syntonically, and with no guilt); by contrast, personality is about who you are holistically speaking (i.e., how you habitually think, feel, behave, relate, desire, attach, etc, but not intentionally). Character can be straightforwardly disordered, most notably, in psychopathic cases (e.g., people who genuinely have no remorse for all the bad things they have done). Personality, however, is a more complex term and thus cannot be straightforwardly disordered (e.g., it is quite impossible that a person has all aspects of their personality, including for instance their hobbies, disordered; it’s more likely that they have a specific aspect of their personality disordered, at which point the term “personality disorder” cannot be used to describe them). In any case, I apologize in advance if this last point sounds pedantic but I wanted to clarify it as this helps me bring my initial “borderline” point back home: “borderline” is not about character (because it’s not something that people do intentionally but instead it’s something that they usually regret after they have done it) and it’s not about personality (because it’s something specific that people do; i.e., it’s not about “all of their personality”). And that’s why borderline is neither a character disorder nor a personality disorder but rather a relational disorder.
Sorbie Richner: Thanks for the in-depth comments. First I’d like to know why you don’t like the word “interpersonal”.
OZ: It’s a pet peeve of mine so may not be so substantive, but here it goes: it reminds me of older interpersonal theorists (like Sullivan) who I don’t like because I think they just re-stated object relations theory and they were not so original (but, to be fair, most people are not original, myself included). More importantly, I don’t like this term as a description of PD because it only deals with what happens between people, but not on what happens between a person and themselves (which is hugely important for self-focused “borderline dynamics” like unstable ways of feeling and viewing oneself). That’s why I think the word “relational” is much better: it’s aligned with classic Freudian theory that distilled character as self-relating (libidinal energy invested in self) vs. object-relating (libidinal energy invested in others), and it’s more flexible, more dialectic, and more enactive because it clarifies what the person with PD is “doing wrong” and could improve on: namely, their ways of relating to both themselves (getting ahead and working better) and to others (getting along with others and loving them better). See here and here.
SR: You nicely defined “character” for the purpose of making the distinction between “character disorder” and “personality disorder”. I wonder if you could expand on the distinction between “character” and “personality”, as they pertain to your work, just a bit more.
OZ: I’ll start with the easy one first: personality. My definition of personality is based on both empirical psychology and psycho-analysis. To begin with empirical psychology, most empirical evidence shows that personality can be distilled in more or less five trait domains (known as the Big Five), namely, neuroticism (tendency to experience negative emotion), openness (tendency to be imaginative and creative), conscientiousness (tendency to be orderly and hard-working), agreeableness (tendency to be compliant and nice towards others), and extraversion (tendency to be outgoing and assertive). In other words: empirically speaking, personality is one’s habitual way of thinking (openness), feeling (neuroticism), behaving (conscientiousness), and relating (extraversion and agreeableness).
Now, psycho-analysis is actually very much consistent with this definition of personality (more consistent than most people would be willing to acknowledge). This is because psychoanalysis also defines personality as one’s relatively stable way of being (including their way of thinking, feeling, behaving, and relating), but expands this definition even further by adding other dimensions such as “ways of attaching to others”, “ways of desiring”, “ways of fantasizing”, “ways of defending the self against anxiety” and so on and forth...
From these points, we can see that personality has at least two properties: first, it is very, very broad (in the sense that it speaks about various dimensions of human experience); second, it is quite stable over time (because it’s about habitual ways of being). Thus, personality can be defined as “how a person tends to think, feel, behave, relate, attach, desire, fantasize, defend, and so on and so forth for all dimensions of human experience”.
That being said, then what is “character”? The answer here is more complex since there are at least two distinct definitions of character. The first one comes from psycho-analysis, with Freud defining “character” as the amount of energy a person invests in themselves (what he called narcissism) vs. others (what he called object-love). Importantly, this distinction was later advanced by Freud’s close collaborators like Wilhelm Reich and Anna Freud who added the idea of “ego-syntonicity”: that is, the idea that these ways of relating to the self and others are consistent (i.e., syntonic) with one’s character. Thus, from this perspective, character is simply “how a person ego-syntonically relates to themselves and others” (i.e., how they relate in ways that are experienced as natural parts of themselves rather than as foreign intrusions that they wish to be cured of).
A second definition of character comes from (moral) philosophy and legal theory. According to this definition, character is one’s moral stance towards others: that is, “how a person treats others, morally speaking”. This is based on traditional philosophical views, most favorably, the one from Theophrastus, who outlined various “character types” that roughly equated with “morally bad ways of treating others” (e.g., the “arrogant man”, who “holds a certain scorn for all the world beside oneself”). This is also based on modern legal theories (such as the one by George Fletcher) according to which a person is held responsible for a crime when their acts express their character: that is, their moral stance toward others (as most crimes are against others).
(One thing to note here is that some legal theories apply the same moral criterion to the self but in so doing end up punishing people who harm themselves, e.g., suicide being criminalized in some countries. Needless to say, I don’t endorse this definition at all so there’s no need to discuss it here.)
In any case, my personal view is that the philosophical definition of character is better than the psychoanalytic one for at least two reasons. First, the philosophical definition only deals with some especially harmful phenotypes (e.g., people who explicitly and intentionally and consistent-with-their-morality harm others) and so, unlike psycho-analysis, it does not treat people with “borderline” or “schizoid” dynamics as having “character disorders”. Second, the philosophical definition is much more honest because it clarifies that whenever we use the term “character”, we are inherently evaluating someone else (i.e., “I dislike this person’s character / moral system”), meaning that we cannot easily divorce the term “character” from its evaluative basis. This is what analysts tried hard to do, but failed as they did not realize that a lot of their theories on “character” were inherently evaluative (e.g., treating homosexuality as a character disorder!). This is also what DSM tried to do and failed even more spectacularly since in order to “de-moralize” the sorts of phenotypes that were under the psycho-analytic rubric of “character”, it replaced the term “character” with the term “personality” and led to a linguistic mess that we are still trying to sort out today…
So, to summarize, I believe that personality is about who someone is holistically speaking (i.e., how they think, feel, behave, relate, attach, desire, fantasize, etc.) whereas character is about who someone is morally speaking (i.e., how they intentionally and morally treat others).
SR: When you wrote about above therapists’ misuse of clinical language as a means of dismissing clients, you were writing about psychoanalytic clinicians’ use of psychoanalytic language1. In the psychoanalytic definition of “character” that you provided, the concept of ego-syntonicity is emphasized; and though you don’t favor this definition for the purposes of your work, ego-syntonicity is certainly a concept that looms large in psychoanalytic settings, especially as it pertains to so-called “personality pathology” and the erstwhile “character pathology”. In the dynamic process I am calling “cliff-falling”, projection, projective identification, and introjection are big players. It seems to me that projective defenses are employed to shore up a person’s self-concept. I wonder if, in such “cliff-falling” scenarios between patient and therapist, the aforementioned misuse of clinical language is to do with therapists’ defending against their ego-dystonic reactions to the experience of “cliff falling”.
Would you please tell a bit about your understanding of the relationship between ego-syntonicity and projective identification within borderline relational dynamics, particularly in a clinical setting? Further, will you please elaborate on why the Freudian-Reichian ego-sytonicity-focused definition of “character” falls short for describing dynamics like these?
OZ: Hmm… You raise a number of interesting but also complex points so I need to be clear in my response to address each of them precisely.
I’ll start with your point on “the relationship between ego-syntonicity and projective identification”. I think this relationship is pretty much non-existent for at least two reasons. First, the language of “ego-syntonicity” comes from Anna Freud and the ego psychology — character traditions; but the very idea of “projective identification” comes from Melanie Klein and, to my knowledge, Klein (and her followers) never described “projective identification” as ego-syntonic or -dystonic. Second, regardless of what these authorities say, the mechanism of “projective identification” cannot logically be syntonic with the self because it is almost always (and almost by definition) unconscious. And if something is unconscious, then it’s never experienced as part of the self and so the person cannot decide whether that’s a desirable or undesirable part of themselves. To illustrate with an example: Suppose that everyone around me keeps telling me “Orestis, you’re a perfectionist”. But suppose that I don’t actually agree with that: I don’t even perceive that as being applicable to myself. In this case, I cannot possibly decide whether this trait is desirable (ego-syntonic) or undesirable (ego-dystonic) because I don’t even agree that it’s applicable to me in the first place! In the same exact way, because everyone who projects is almost always unaware they are projecting, they cannot experience the projection as syntonic or dystonic at all. They simply experience it as completely irrelevant to themselves.
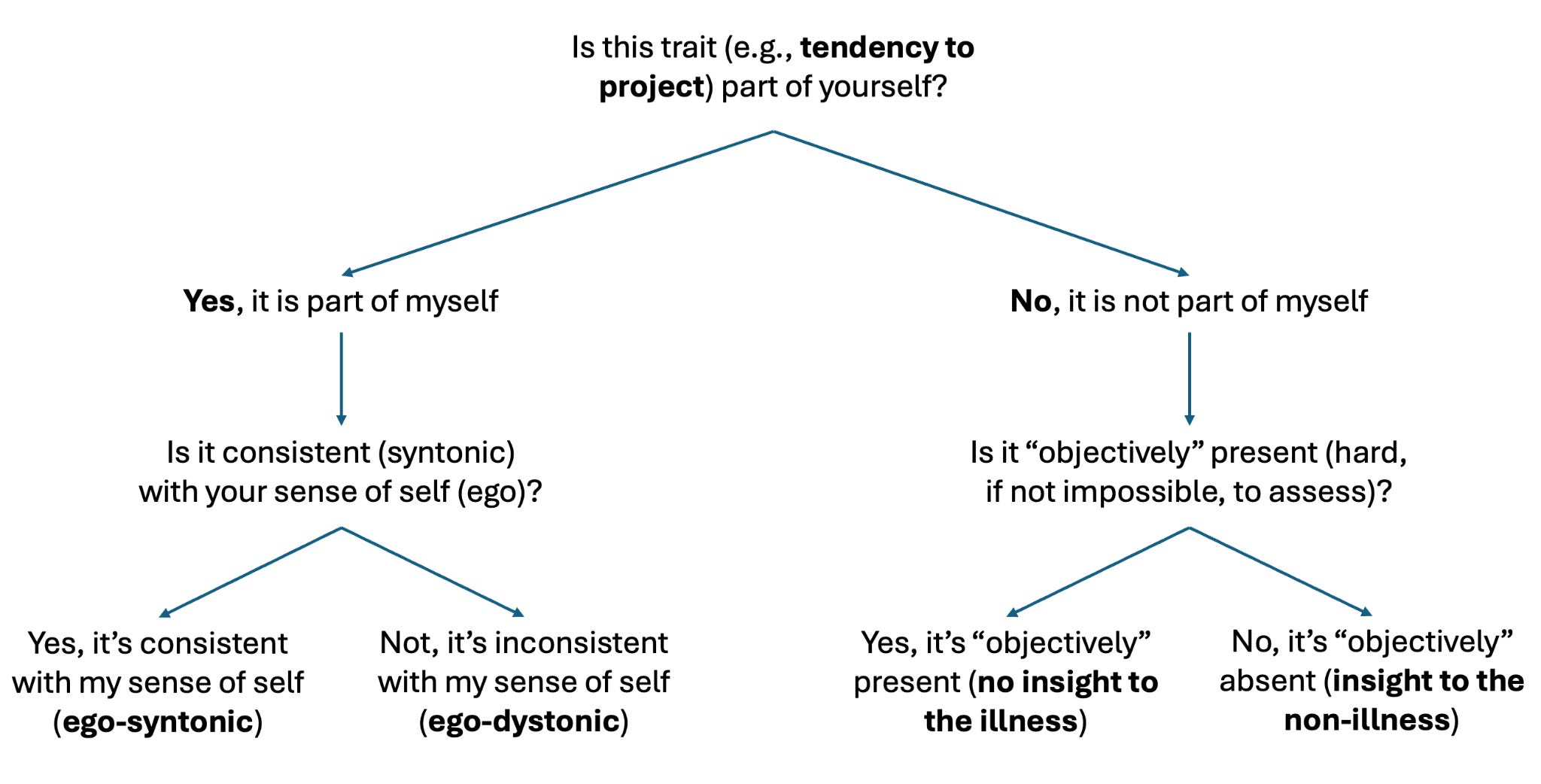
Now, a problem here might be that a clinician comes and says “The very fact that you’re denying this, and you experience it as irrelevant, still means your problems are ego-syntonic.” This (very predictable but unfortunate) statement, however, still fails logically because it’s not really talking about ego-syntonicity but about “insight into the illness”. Again, ego-syntonicity is simply “I acknowledge this trait as part of myself and I believe it is consistent with myself.” But notice how “denying a trait” rejects the very first part of this definition: the moment I deny that I even have an experience (say, I deny that I have a delusional belief), then I cannot answer the question “Are my delusions consistent with my sense of self or not”, since again, I don’t even experience them as part of myself! So, as soon as the person rejects something, they are no longer in the realm of ego-syntonicity but in the realm of “insight” (as in “Do you have insight to a putative illness?”), which is sometimes unfortunately conflated with ego-syntonicity but which needs to be kept separate because it’s another intricate issue of its own (see Figure 1).
Finally, I’d like to note the only correct use of ego-syntonicity, in my opinion, which is when ego-syntonicity is applied to conscious, not unconscious material. To illustrate, consider two adolescents, both of whom are delinquent and both of whom are consciously aware that they are delinquent (i.e., they accept that’s a part of themselves). One, however, finds this pattern ego-dystonic because they’re involved in a strange relational dynamic within a gang setting; whereas the other finds this pattern ego-syntonic because they are happy being delinquent. Obviously, the first person has a better prognosis and this is a nice illustration of how ego-syntonicity can be usefully applied to separate “relational dynamics” from “character dynamics”. But notice how in this case the material being analyzed is fully conscious and clear, whereas the material analyzed in the previous cases are more unconscious and thus less clear. This is, I think, the key thing to correctly using the criterion of ego-syntonicity: namely, to apply it onto clear and conscious traits that a person sees as part of themselves. To the extent that something is not even experienced as part of the self, then it cannot be evaluated as being syntonic or dystonic with the self—and the task then would be to figure out first whether that aspect is indeed part of the self (i.e., “I did project yesterday”) or not (“I never projected”) and then decide whether it’s syntonic with the self (i.e., “I was right to project”) or not (i.e., “I was not right to project and I feel guilty because that’s ego-dystonic”) (see Figure 1).
Now, all that being said, I think it becomes quite obvious why the concepts of “ego-syntonicity” and “character” etc are not really applicable to “unconscious borderline dynamics”—again, because these dynamics are unconscious, they are not even being viewed as part of one’s self, and they are thus unable to be evaluated as being syntonic or dystonic with the self. Which begs the question then: How are these dynamics best understood, if they cannot be understood using these traditional concepts? I think the best way to understand the specific “unconscious, borderline dynamics” you are mentioning is through the lens of Bion, my absolute favourite psycho-analyst. If you allow me, I will expand below on why I think Bion’s model is the most accurate model with regard to conceptualizing “unconscious borderline dynamics” like projection, identification, etc.
To begin with, let me start by clarifying that according to Bion, “projective identification” is not really a defense. It’s also not an inherently pathological process. Instead, it’s a developmentally necessary process. To briefly elaborate, the key Bionian idea is that infants engage in a lot of “projection”, not because they hate their caregivers and not even because they want to defend themselves. It’s more like they want to “regulate themselves” by “evacuating” unbearable feelings into their caregiver. If the caregiver is “good enough” (as per Winnicott), then what they will do is take these “projected affects” and “contain them”: that is, they will hold the baby, they will soothe the baby, and they will NOT strongly identify with the projected affects (and thus not act on them), because they will appreciate that those projected affects are not “attacking them” per se; rather, these raw affects exist (now within them) because the person (baby) in front of them cannot possibly bear them and they need help containing them.
Beyond containing these affects and not strongly identifying with them, the “good enough” caregiver must also engage in a process that Bion called “alpha function”, which is just a fancy term to say that the caregiver needs to take these raw affects (what Bion called beta elements) and transform them into more symbolic mental elements (what Bion called alpha elements), which are more “thinkable” and more “palatable” to the infant. A useful analogy here is when a mother bird takes raw, hard food that her chick cannot yet swallow, chews it into something soft and digestible, and feeds it back to the chick. That’s what a “good enough” caregiver (and also, therapist, but more on this later) does: they “chew” on the projected raw affects, they transform them into more symbolic mental elements, and they then put them back into the baby in order to gradually enhance the baby’s capacity to perform this kind of “symbolic” or “alpha” or “reflective” or “mentalizing” process themselves: that is, whenever they are in distress to not project or externalize or evacuate their affects, but to contain and think and reflect on them.
Now, as you can see this Bionian model is vastly different from other “defensive” or “character-based” views of “projective identification” because it emphasizes repeatedly that “projective identification” is not simply “baby projects and caregiver identifies” but rather “baby projects and caregiver identifies just enough so that they can contain the baby’s projection”. So, the whole point of Bion is that “projective identification” is a form of internal regulation and external communication: the baby cannot regulate itself and it’s trying to communicate to the caregiver its unbearable affects so that the caregiver can contain them.
I think what’s wrong with a lot of recent (formal and informal) discussion around “projective identification” is that it often neglects this basic fact: the projection is not happening because the patient is trying to harm people or because the patient is trying to make the therapist behave in a bad way; rather, the projection is happening because the patient is trying to communicate something. And the therapist’s job is to NOT take that communication personally (i.e., to strongly identify with it and act on it). In fact, the moment a therapist strongly identifies and acts out on a projection, the game is likely already lost. That’s why supervision is so important since the entire point of supervision is to give the therapist also a chance to evacuate and to project unbearable affects onto someone else (their supervisor, not the patient!). And the supervisor is supposed to take in those affects, and metabolize them, and then transfer them back (in a more palatable format) to the therapist so that the therapist can in turn make sense of them and return to therapy ready and re-energized to contain more unbearable affects from their patient.
Therapy is not easy and it’s particularly not easy when the patient is extremely emotionally unstable because they’ve never had a figure in their lives to help them contain their emotions. So, the whole point of therapy (not only for “borderline” patients but for all patients) is for the therapist to act as a container: they need to remain calm enough, and neutral enough in order to gracefully receive the projections, identify with them “just enough” so that they can understand them, contain them, then metabolize them, and then return them back to the patient in a more palatable and thinkable form. And this is a lot to ask of a person but that’s the job…
Yet, unfortunately, this job is not being done well by some people, which is why we see some online discourse where therapists use the term “projective identification” to excuse themselves for not being “good enough” in containing their patients’ emotions. I don’t want to point fingers at particular people because I think this finger-pointing process is precisely the root of the problem: person A projects, person B identifies (i.e., gets triggered), person B then projects what was not contained well, then person A gets further triggered and projects even further, and so on…
I think to end this cycle of “cliff falling” or “perpetual projection, identification, and re-projection”, we need to bring the Bionian model into the forefront: that is, we need to re-frame “projection” and “identification” and all other unconscious processes as neither “defensive” nor “inherently pathological” and nor even “ego-syntonic” but rather as things that are “universal” and serve the function of “regulating ourselves” and “communicating to others”. Only when we reframe these processes using this more humane language will we appreciate that they exist within us all — and only then will we be able to help each other metabolize what we cannot alone contain.
SR: Thank you!
Here I would urge readers to read Mr. Zavlis’ paper “The dangers of reifying ‘borderline personality disorder”, in which he argues that psychoanalytic language should not be weaponized to deflect criticisms against the idea of borderline personality disorder.
Excellent, I loved this! Thank you Sorbie and Orestis. Orestis, one question for you. Where does this idea come from, that in order for “personality disorder” to apply, “all aspects” of a person’s personality should be disordered? We don’t really apply this sort of rule to other problems. Eg, if someone has a “movement disorder” or “neurodevelopmental disorder” that doesn’t mean that all aspects of their movement or neurodevelopment should be disordered. Why cannot “personality disorder” apply to “some aspects” of personality?
This interview is the first time that I actually even understood what the projective identification that previous misapprehension posts described, because to me the role of the therapist described by Orestes Zavlis is obviously obvious. I mean, if the therapist doesn't do that in terms of containing the client's emotions, then what are they even doing? I struggled with the concept of cliff falling, and I still don't quite understand what it was meant by that, but this clarified a lot for me.
But I've got a question about ego syntonic versus dysonic, because there is something I don't understand. What if a person accepts that something is part of them very much (descriptively), but it's broadly undesirable? Is that syntonic or dystonic? Surely a lot of stuff is like that. For example I'm kinda ADHD scatty mentally, loud in volume and physically fat. I don't love those things, I'd rather dial them down (not remove) but they're OBVIOUSLY me.